
VIEWING BONES THROUGH TELESCOPES
Probably primitive
man's curiosity markedly increased soon after he stood up and started walking
on just his feet. He could both peek into caves and drop back onto all fours to
peer down badger holes. Looking into his family’s mouths and ears soon
followed. Many generations later his progeny developed metal tubes and glimpsed
human interiors through all of our natural orifices. Lighting, however, was
always an issue, and the torch that satisfactorily illuminated the cave was poorly
accepted by early patients in the proctology clinic. FIGURE
1

This changed in 1879
with Edison’s invention of the incandescent light bulb. Just seven years later,
two German doctors were lighting up bladders with a tiny bulb on the end of a
steel tube through which they squinted. Heat from the bulb and risk of
breakage, however, posed problems. Nonetheless, enterprising doctors began
poking holes in the skin and exploring the bladder, abdomen, and chest with
lighted tubes. In 1912, Severin Nordentoft, a Danish doctor, extended this
concept to the knee and coined the word “arthroscopy” (joint-view). Multiple
investigators from the world around then refined and continue to refine the
technique.
Prior to antibiotics,
tuberculosis, especially in the knee, occupied much of orthopedists’ time. This
was particularly so in Japan, where squatting and kneeling have long been
cultural imperatives. In 1918 Doctor Kenji Takagi began using a bladder scope
to examine tuberculous knees. His idea was to develop early treatment that
would preclude the awkward outcome of an entirely stiff knee. Over the next 20
years he designed and tested 12 versions of arthroscopes that were
progressively smaller in diameter and that incorporated better optical systems.
None of them, however, were entirely practical.
After World War II,
Takagi’s student, Masaki Watanabe, took up the banner and continued to make
design improvements. In 1957, Watanabe presented a color movie describing his
work, first to an international orthopedic meeting in Spain and then to major
European and North American orthopedic groups on his way home to Japan. The
response was tepid at best.
Undaunted, Watanabe
pressed on. The twenty-first version finally provided an adequate view and good
focus even though it necessitated grinding each lens by hand. By 1958 this
version became the world’s first production arthroscope, but breakage of the
incandescent bulb on the end of the tube continued to be problematic. Watanabe
began to receive international visitors interested in learning his technique;
but when they returned home, began using it, and reported their results,
collegial criticism, even ridicule, prevailed.
In 1967 the
twenty-second version, for the first time, incorporated a novel fiber optic
cable. Now the hot, fragile light bulb could be 6 - 10 feet away from the
operative field and transmit “cold light” into the knee joint via thousands of
bundled glass threads.
Watanabe
developed at least three more versions to further address the conflicting goals
of better illumination and visualization vs. smaller diameter scopes that could
probe the deepest recesses of small joints. His final version was less than
1/12th of an inch in diameter—about the
diameter of a coat hanger wire. Later came miniaturized television
cameras that could be attached to the arthroscope. A video monitor in the
operating room displayed the images. Now residents, nurses, and students no
longer had to stare at the back of the surgeon’s head as he squinted into an
eyepiece attached to a narrow tube. Patients, when awake, could watch too, and
a video recording of the event later allowed their families untold hours of
viewing pleasure. Well, maybe minutes.
Along with further
advances in arthroscopic instrument and in scope design, international interest
began to grow. At first, every procedure was merely diagnostic and was followed
immediately by a large incision and exploration of the joint under direct
vision to treat whatever pathology the arthroscope had revealed.
Tiny nippers and
shavers, first manual and then also powered, began to allow for arthroscopic treatment as well as diagnosis.
Current techniques and instruments even allow the surgeon to place and tie
sutures inside a joint. Such minimally invasive surgery allows for faster and
more complete rehabilitation. Because the knee joint is large, the innovations
started there, but now orthopedists also routinely apply these techniques to
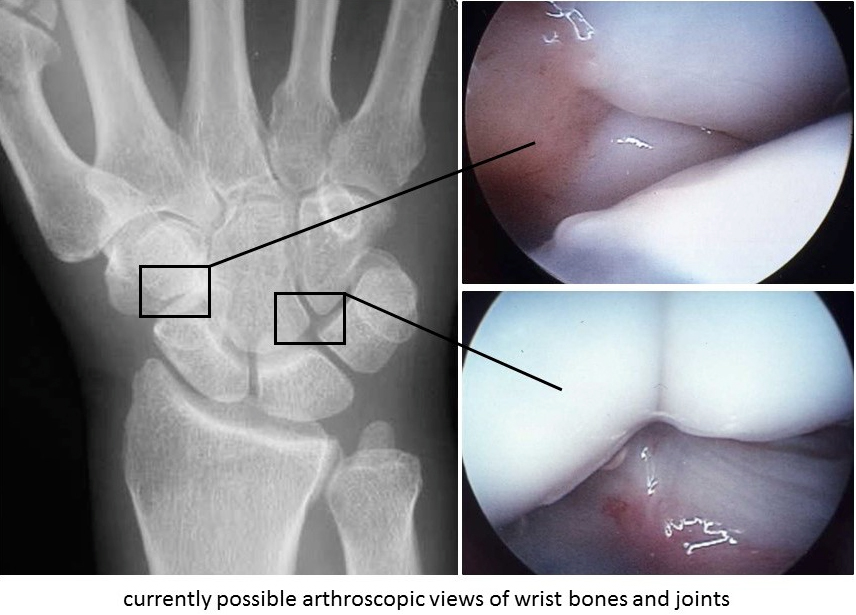
the shoulder, elbow, wrist, hip, and ankle joints. Undoubtedly our caveman ancestors,
torches and clubs in hand, would be pleased to know where their curiosity for
peering into holes has led. FIGURE 2
Sources:
Jackson RW: A
history of arthroscopy. Arthroscopy 2010; 26 (1): 91–103
Spaner SJ, Warnock GL: A brief
history of endoscopy, laparoscopy, and laparoscopic surgery. J
Laparoendosc Adv Surg Tech A. 1997;7(6):369-73.
Treuting R: Minimally invasive orthopedic
surgery: arthroscopy. Ochsner J 2000; 2(3): 158–163.